No-reflow on abdomen CT
60 year old F had acute onset of severe right-sided chest pain while watching TV. Prehospital providers noted STEMI and activated the cath lab. Culprit for acute anterior STEMI was a ruptured plaque in the proximal LAD with 95% thrombotic stenosis stent placed with excellent angiographic result. In other words, complete restoration of flow through the LAD.
The next day she had abdominal pain and a CT scan of the abdomen and pelvis was performed. There was no acute finding in the abdomen, but the cuts through the lower chest showed interesting findings in the LV. On 40 keV monoE and iodine map, there is a large perfusion defect in the LV corresponding to the LAD territory. This is better seen on short-axis view. On spectral CT, this is a slam dunk, while on routine CT it would be quite a stretch to make this call.
Now we know she had an outstanding angiographic result, so why is the myocardium not perfused? The reason is microvascular obstruction, a well know phenomenon to cardiac MR readers. This is usually seen in delayed presentation and often indicates a bad prognosis. Our patient struggled for some time and had a troponin peak of about 260(!!).
This case highlights the importance of reviewing the images through the heart on all CT scans, and using spectral images to diagnose perfusion deficits with high confidence.

EKG at presentation: The ST elevations are remarkable, and can be diagnosed by a radiologist
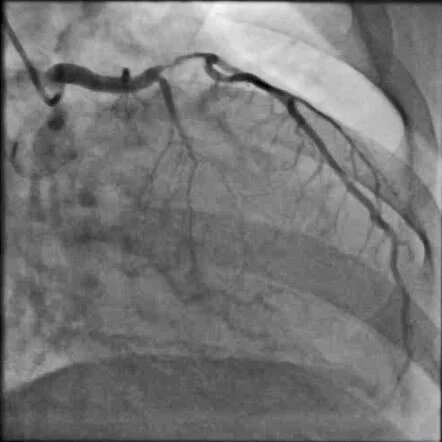
Angiogram shows severe LAD stenosis with thrombosed plaque

Post-stenting: Absolutely gorgeous result!
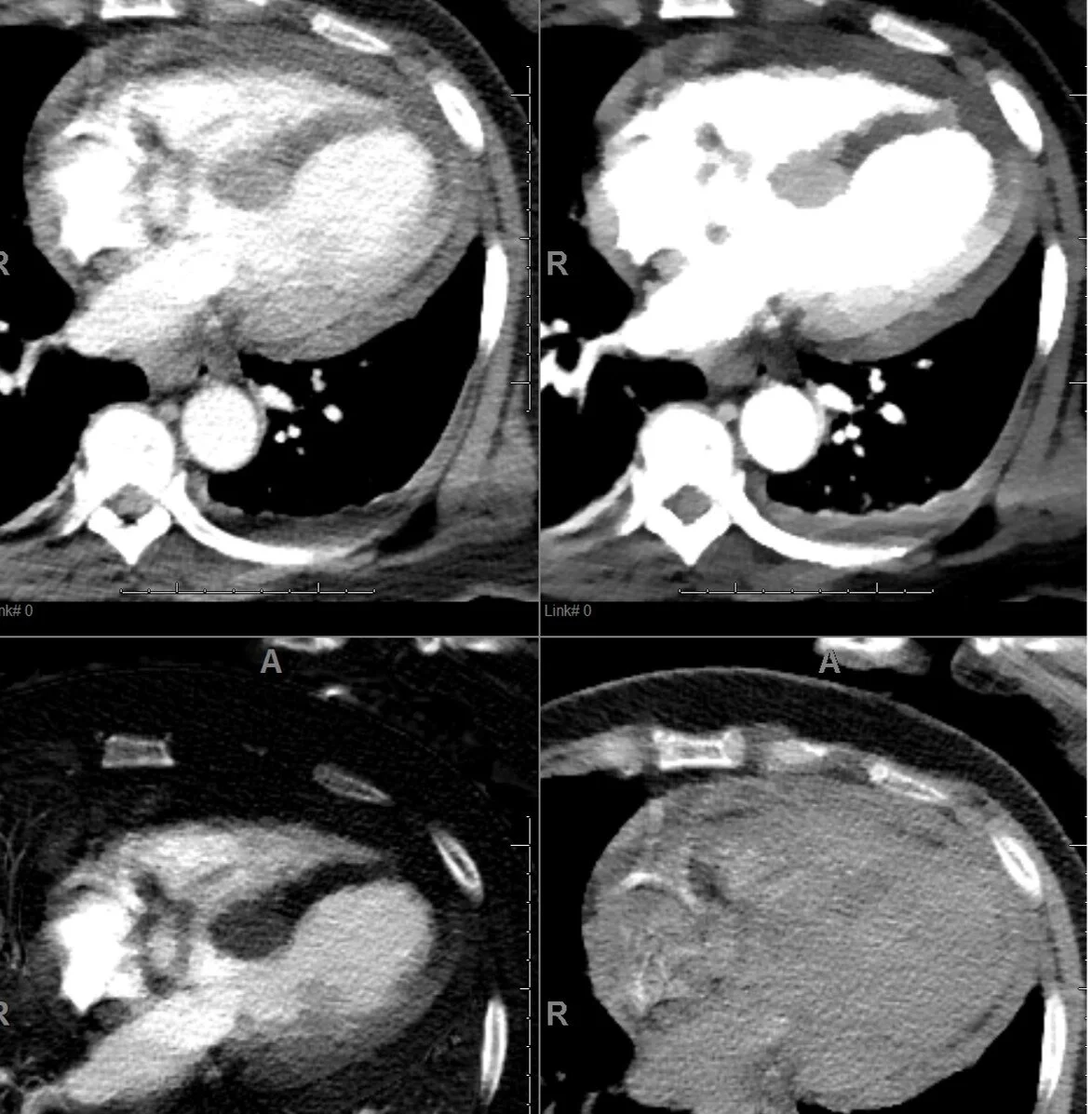
PACS screengrab: Large hypoperfusion in LAD territory best seen on iodine map (left lower image) and 40 keV (right upper image).
This is routine where I work: Spectral recons are sent to PACS, and do not need a special system to review.

Conventional CT: short axis. You might call the perfusion defect, if you were lucky and having a good day.
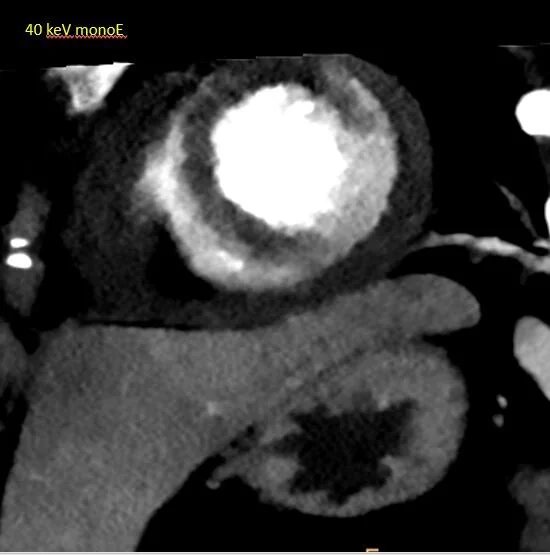
40 keV monoE: Impossible to miss
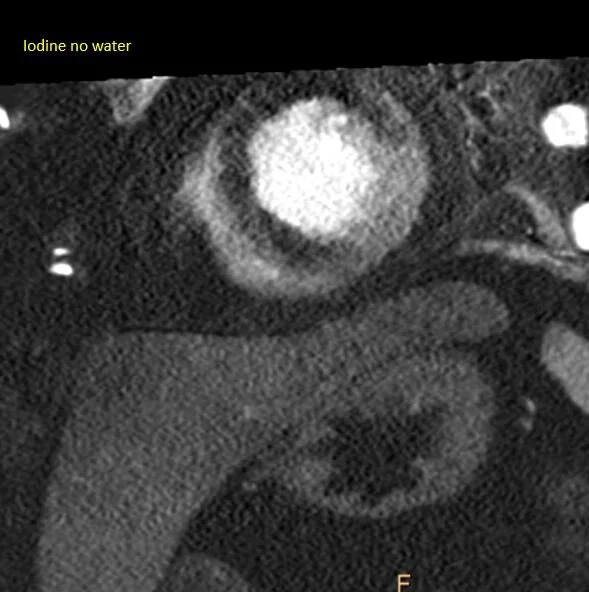
Iodine map
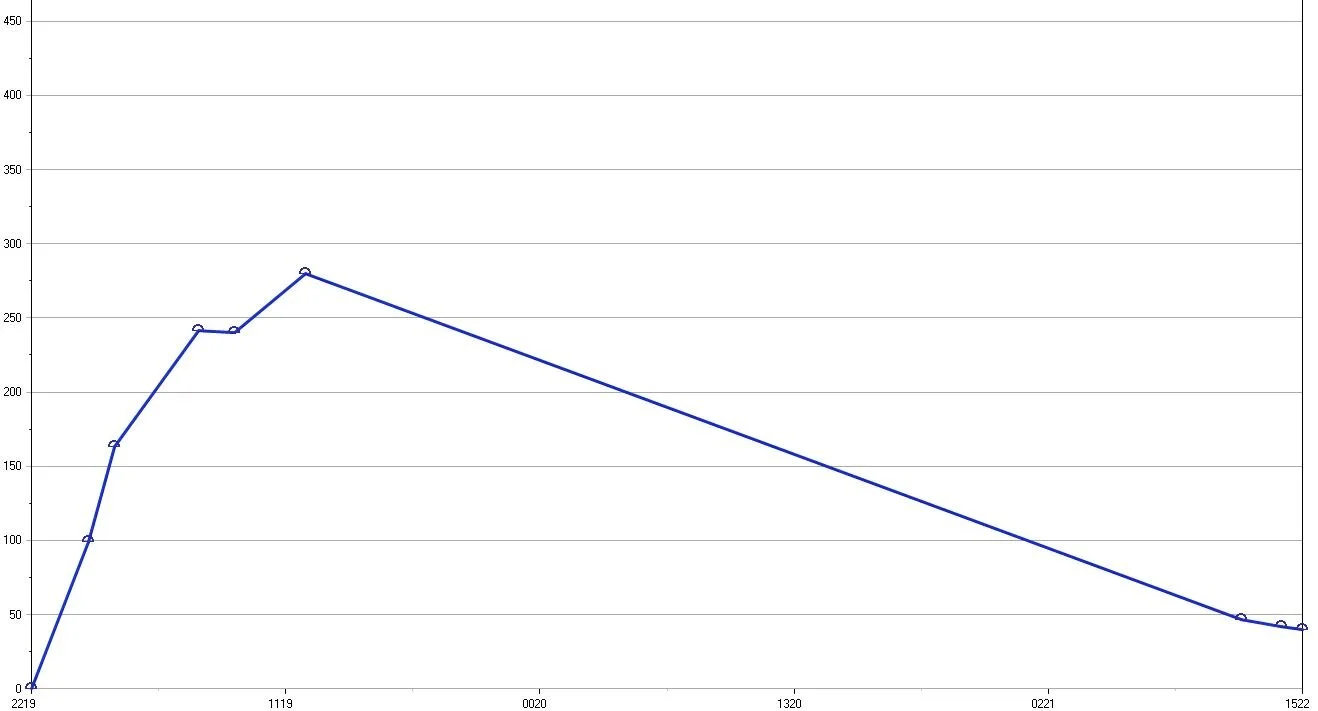
Troponin curve: Rare to see a troponin peak this high in my limited experience.
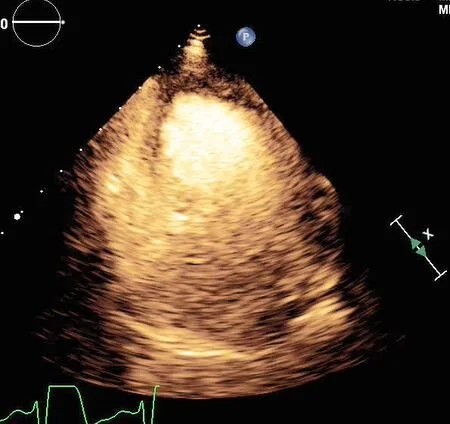
Contrast echo confirms the perfusion defect