A mystifying nodule
60 year old M presents with enlarging “subcarinal” nodule.
A few years ago, he was diagnosed with a large right renal cell carcinoma, with tumor thrombus in the right renal vein. Nephrectomy performed and showed a clear cell carcinoma, with clear margins.
Two years after diagnosis, a tiny right lower lobe lung nodule was discovered, which progressively enlarged on followup. No other lesions on workup. On FNA and subsequent resection, this was a lung metastasis from RCC.
Another two years later, a “subcarinal” nodule was noted, which had been gradually getting bigger. A metastasis was suspected, and FNA performed. Path was negative for malignancy. So FNA repeated, and again negative. Now what?
Spectral CT gives a clue. The nodule is intensely enhancing, with very high iodine uptake. Combined with the location of the nodule in the roof of the left atrium, a cardiac paraganglioma was suspected. A gallium 68 dotatate scan performed, which shows intense uptake in this nodule, confirming the diagnosis.
Cardiac (or more appropriately paracardiac) paragangliomas are supposedly very rare tumors, although I have seen several over the years. They can sometimes be functional or malignant. The tumors are intensely vascular, which is a clue to diagnosis, and they are sometimes incidentally discovered on coronary angiography. The roof of the left atrium is a favored location, as in this case, which may have to do with the distribution of cardiac autonomic nerves. Treatment is surgical, although some can be observed safely.

Conventional CT many years ago shows large right kidney mass
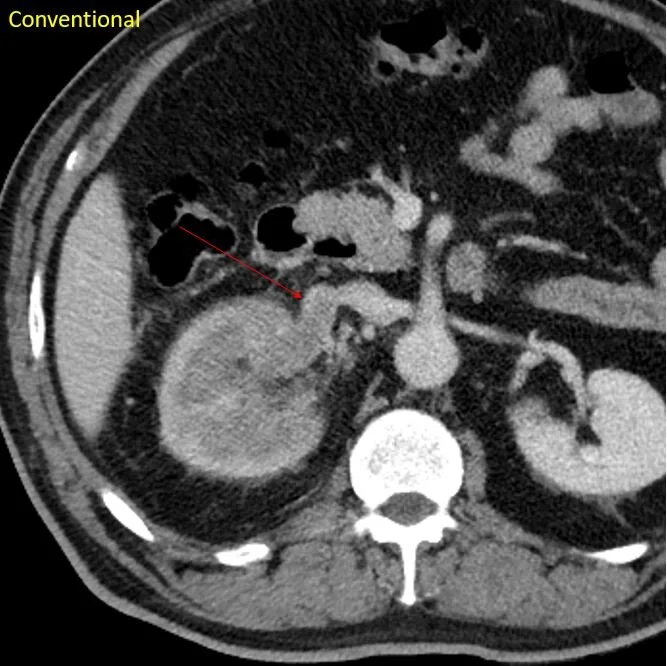
Tumor thrombus in right renal vein (arrow)
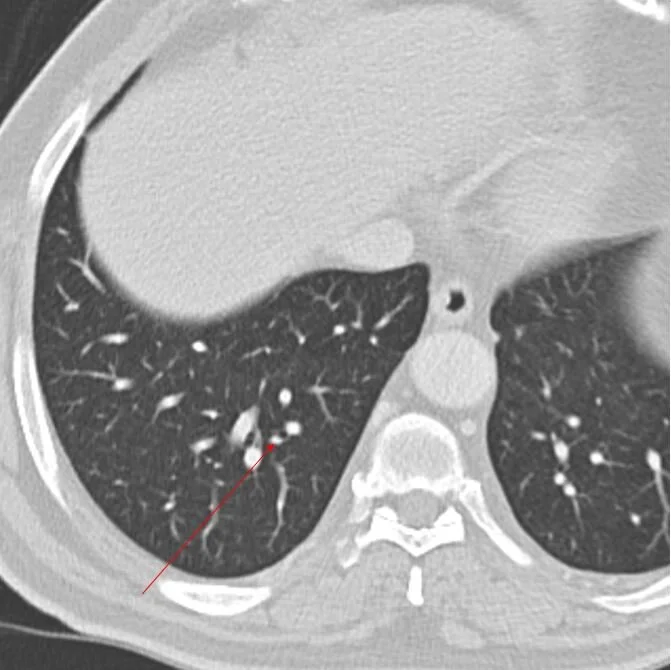
CT 2 years after nephrectomy. Tint RLL lung nodule.
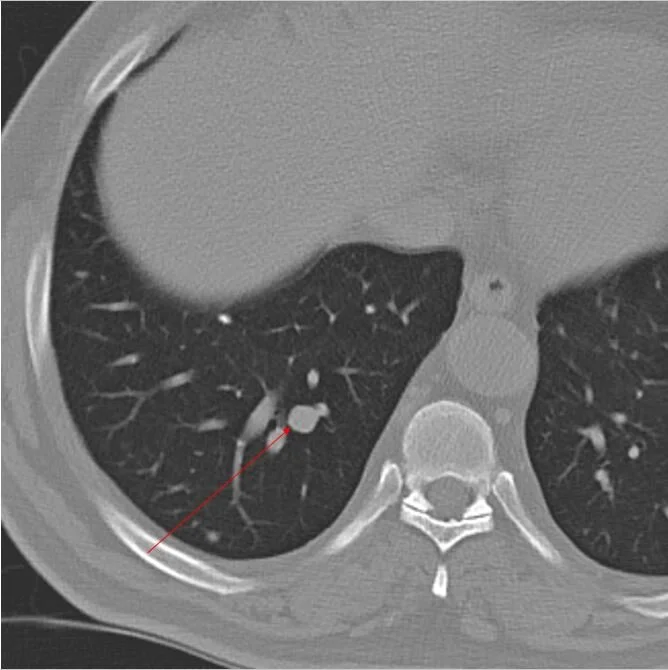
Followup CT 1 year later, nodule is larger. This was oligometastasic disease.
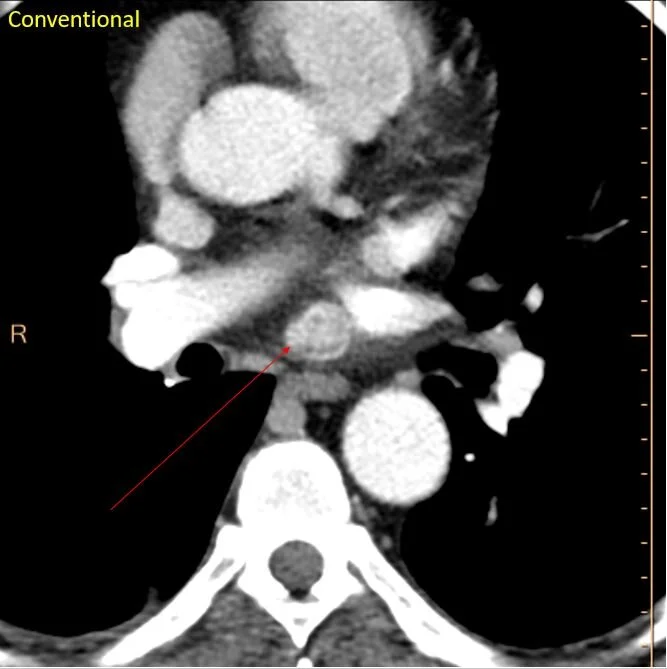
CT a couple of years later. Intensely enhancing subcarinal nodule.

The subcarinal nodule has intense uptake on iodine map.
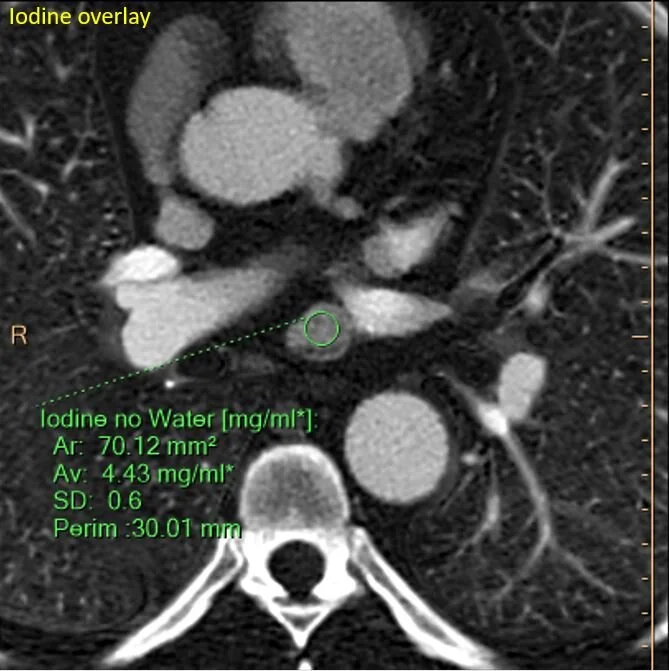
Quantitatively intense iodine uptake.

Image captured from EUS FNA. They nailed it!
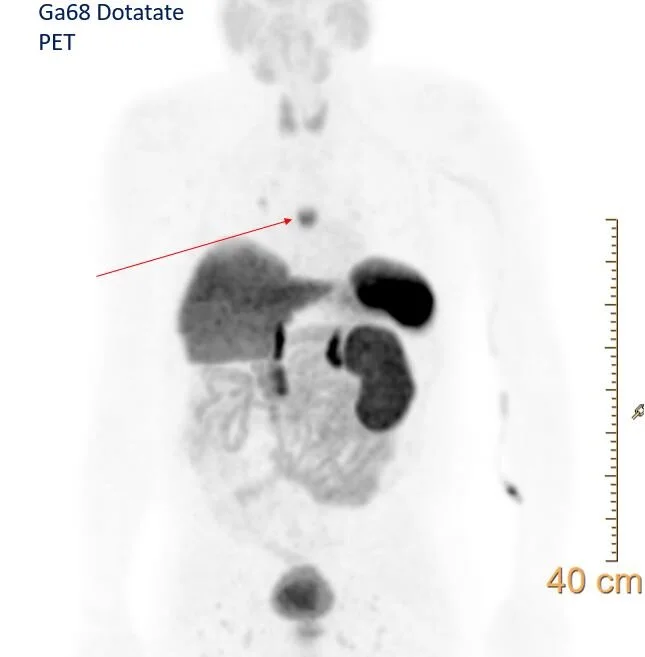
Dotatate scan: The nodule shows uptake, consistent with neuroendocrine tumor. Note physiologic uptake in the spleen, adrenals and kidneys, as well as uncinate process of pancreas.
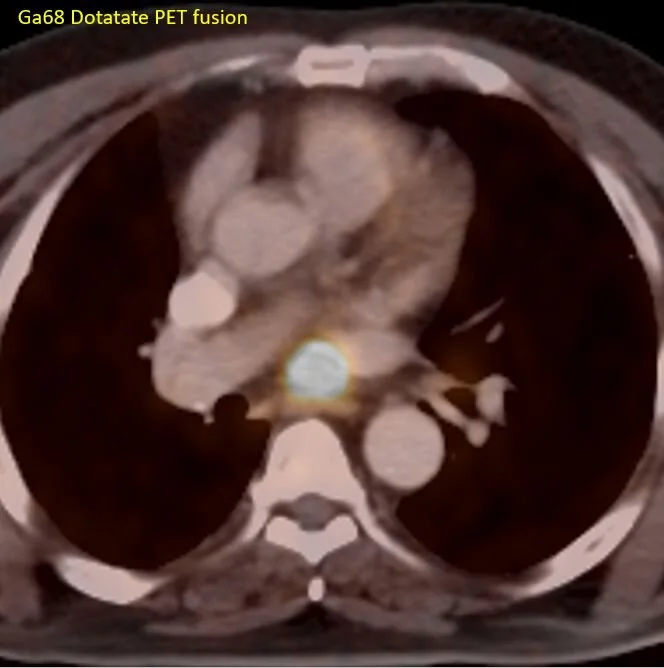
Fusion image confirms uptake in the subcarinal nodule.

Coronal image shows the nodule is in the roof of the left atrium.