Matters of the heart
66 year old male presents awake and answering questions after MVC. FAST ultrasound shows a hemopericardium. CXR unremarkable. Intermittently hypotensive. CPR started after pulses lost in spite of maximal resuscitation. Return of spontaneous circulation after one round of ACLS.
An EKG was done. This showed ST elevation in inferolateral leads and reciprocal elevations. Hemopericardium remained stable. A CT scan was then performed, with the suspicion of a type A dissection.
Conventional CT shows no aortic dissection. There is a large hemopericardium, as expected, and a filling defect in the LV apex consistent with thrombus. On spectral analysis, the apical clot shows no uptake of iodine. Interestingly, there is also lack of iodine uptake in the inferolateral wall, consistent with an acute MI.
The very astute radiology resident obtained delayed images through the chest. The inferolateral wall shows absolutely no iodine uptake, confirming the acute MI. The absence of iodine uptake is much easier to appreciate on delayed images. Very subtle increased uptake in the aneurysmal LV apex around the clot, suggests an old MI with delayed hyperenhancement and scarring.
Troponin came back at 74. The hemopericardium? Not sure, but it was likely from a spontaneous rupture that closed, or was plugged by clot at the time of imaging. Patient subsequently re-arrested and unfortunately could not be revived.
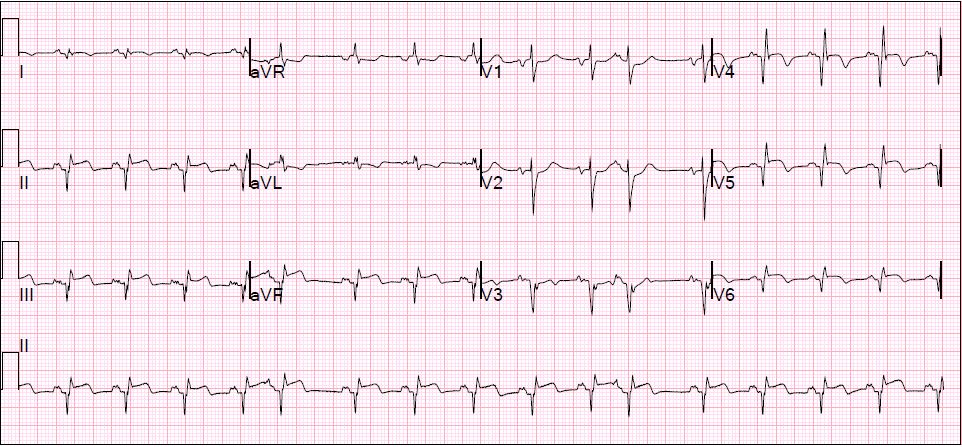
EKG: Very important for radiologists to appreciate the inferolateral MI (just kidding).

Conventional trauma CT: Note hemopericardium and filling defect in the LV apex.

Iodine map: LV apical clot without iodine uptake. Can you appreciate the hypoperfusion in the inferolateral wall? If not, delayed images below make it much more obvious.

Fused iodine map, early scan: LV apical clot and inferolateral hypoperfusion.

Conventional delayed scan. This is key in making the diagnosis.

Delayed image, 40 keV image. Iodine is a lot brighter, so the clot and MI are both much more obvious.
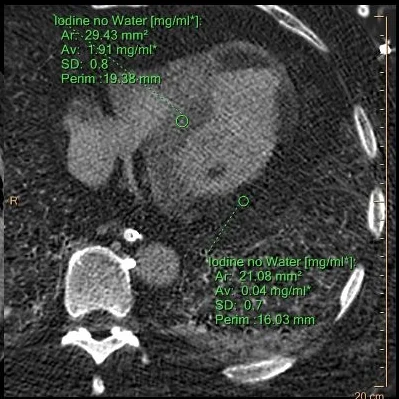
Delayed scan, iodine map: Uptake in inferolateral wall nearly zero. Uptake in septum approximately 1.9 mg/mL for comparison. Notice the very subtle increased uptake in LV apex, likely from a previous MI and scarring.
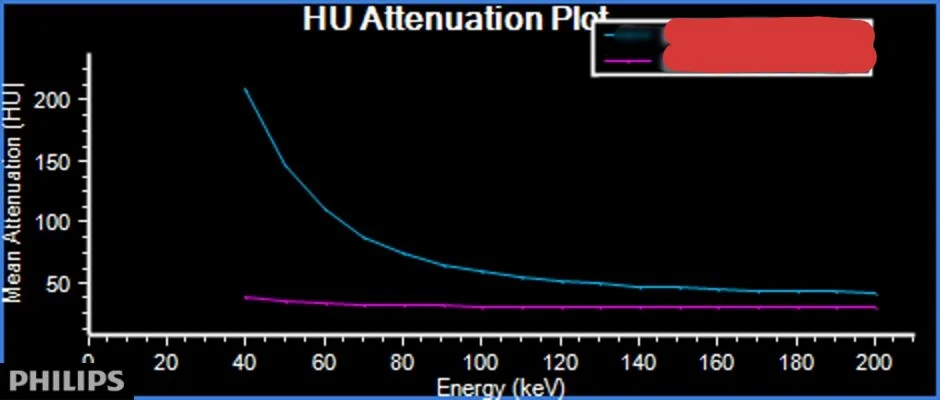
Spectral plots on delayed image: Magenta curve from an ROI on the MI is flat, consistent with lack of iodine. The ROI in the interventricular septum shows significant increase on lower keV, consistent with iodine uptake.
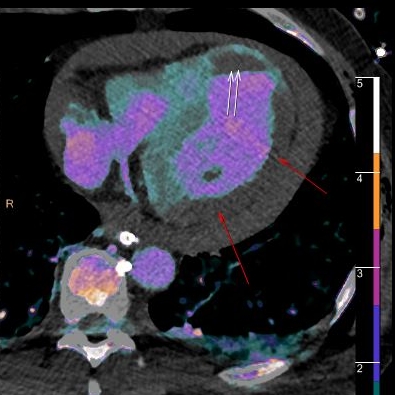
Fused image with iodine overlay: white arrows show the LV apical clot. Red arrows highlight the acute inferolateral MI.